

The knee arthroscope is one of the most commonly performed surgical procedures in Australia, with over 100,000 surgeries performed every year (and reportedly around 700,000 cases a year in the US). Some very interesting research (and quite troubling for the surgeons) is failing to show the benefits of the arthroscopic intervention for meniscal tears, and perhaps most importantly, some studies are indicating that sham surgery (where a patient has an arthroscope, but absolutely no surgical/reparative work performed), is as good or better than the real surgery (where the meniscus is actually repaired or resected).
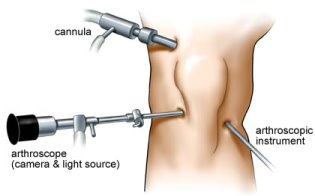 First, a definition – the term “arthroscope” does not refer at all to the work that is completed inside your knee. The arthroscope is merely a form of entry into your knee, done via very small incisions (often called keyhole surgery). So two people can both have arthroscopes performed, but one has had a very minor 20 minute clean out, whilst the other has had a two hour extensive repair – obviously effecting their outcomes and rehabilitation times. This lack of understanding forms the basis of one of the more frequent questions we get asked by patients: “My neighbour had an arthroscope and he was back playing football in 3 weeks, why has it taken me three months”?
First, a definition – the term “arthroscope” does not refer at all to the work that is completed inside your knee. The arthroscope is merely a form of entry into your knee, done via very small incisions (often called keyhole surgery). So two people can both have arthroscopes performed, but one has had a very minor 20 minute clean out, whilst the other has had a two hour extensive repair – obviously effecting their outcomes and rehabilitation times. This lack of understanding forms the basis of one of the more frequent questions we get asked by patients: “My neighbour had an arthroscope and he was back playing football in 3 weeks, why has it taken me three months”?
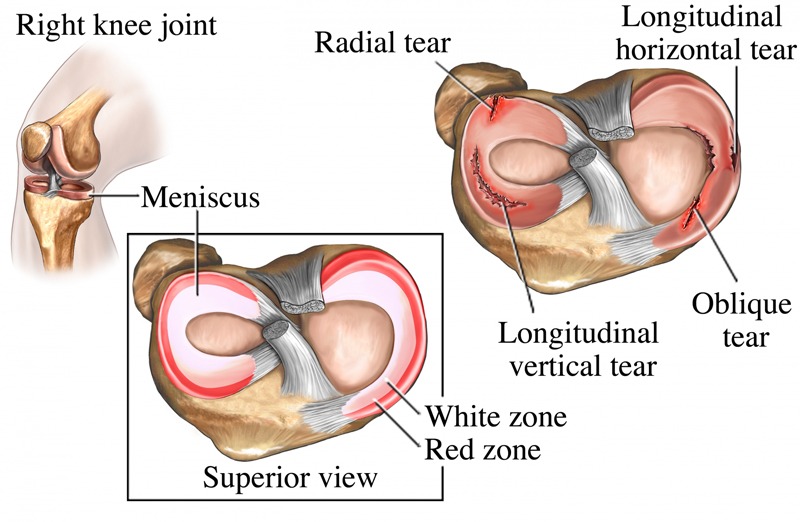
What is the Meniscus?
The meniscus (commonly referred to as “cartilage”) is a natural shock absorber that sits between the femur (thigh) and tibia (shin) bones, helping not only to absorb weight bearing load but also to provide some stability for the joint.
 Over the course of our lives, the meniscus absorbs enormous loads (as it is designed to do) so it is only natural that as we get older, the meniscus starts to show degenerative changes and not uncommonly, tears. As one article so elegantly states: “meniscus tears in middle age are like wrinkles – everybody has them”! One study in Massachusetts concluded that just as many middle-aged people without knee pain had meniscus tears as those with knee pain! In fact the study showed that 61% of people with meniscal tears on MRI had NO pain, aching or stiffness in the joint! This is not unlike the rotator cuff tendons in the shoulder – research shows us that up to 60% of people over 60 years of age will have evidence of shoulder rotator cuff tears on scan. Yet many of these people are completely asymptomatic, in fact it is thought that approximately 75% of people with rotator cuff tendon tears do not require surgery at all.
Over the course of our lives, the meniscus absorbs enormous loads (as it is designed to do) so it is only natural that as we get older, the meniscus starts to show degenerative changes and not uncommonly, tears. As one article so elegantly states: “meniscus tears in middle age are like wrinkles – everybody has them”! One study in Massachusetts concluded that just as many middle-aged people without knee pain had meniscus tears as those with knee pain! In fact the study showed that 61% of people with meniscal tears on MRI had NO pain, aching or stiffness in the joint! This is not unlike the rotator cuff tendons in the shoulder – research shows us that up to 60% of people over 60 years of age will have evidence of shoulder rotator cuff tears on scan. Yet many of these people are completely asymptomatic, in fact it is thought that approximately 75% of people with rotator cuff tendon tears do not require surgery at all.
Yet for some reason it has long been thought that if you have knee pain, AND a meniscus tear is shown on scan, that the only way out is arthroscopic surgery to repair the meniscus (keep in mind though that the surgery is often not actually a “repair” but rather a “resection” of the torn fragment of cartilage. In other words, although the torn fragment is no longer there (meaning you probably feel a definite improvement) you have a lost a percentage of that critical shock absorber. Greater than 90% of arthroscopic meniscal surgery involves resection, NOT repair.
Imagine your meniscus like the shock absorbers in your car – as the cars shock absorbers got thinner and thinner, imagine if all we did was cut a chuck out of the worn shock absorber – probably wouldn’t fix the problem and would actually more than likely hasten the wear and tear on the rest of the car. There is some definite evidence that meniscal surgery, like cutting the chuck out of the worn car shock absorber, may actually lead to acceleration of degenerative change in the knee, and result in earlier onset arthritis in the joint.
What Do The Studies Show?
The first flags seem to have been raised in 2002(1) when a study by a Baylor College of Medicine orthopedic surgeon showed that debridement (the cleaning up of a knee that has arthritis and degenerative meniscus tears) was no better than a placebo.
In 2012(2) a large high-level research study published in the New England Journal of Medicine showed that on average, patients who had meniscus surgery didn’t do any better than those who skipped the surgery and just had physical therapy. Many orthopedic surgeons criticized the study by saying that these patients had some arthritis and that there was still a justification for performing the procedure on patients with a meniscus tear without arthritis.
This theory however, seemed to be disproved by another high level study in 2013(3), that compared meniscus surgery and sham surgery in patients with a meniscus tear but without arthritis. The outcome? One year later, both groups reported equally favorable responses to the procedure—primarily, reduction in knee pain. In the end, the researchers concluded that the real knee surgeries offered no better outcomes than the sham surgeries.
It seemed there was still one condition left where meniscus surgery might be helpful—a meniscus tear that was causing locking of the knee, however this was disputed by the most recent study out of Finland(4), testing the benefit of arthroscopic meniscal surgery on patients who had “mechanical symptoms” (i.e., locking or catching thought to be caused by the meniscus). Half of these patients had real meniscus surgery, and about half got a sham surgery. What was quite staggering was they found that the surgery provided no benefit to relieve knee catching or occasional locking.
What about patients with severe frequent locking of the knee or younger patients who have an acute meniscus tear? Perhaps there is a role for meniscal surgery in some cases, but given the mounting evidence regarding not only the (lack of) effectiveness of the surgery, but also that studies have shown the risk of rapid onset of arthritis and increased forces on the cartilage after a meniscus surgery, it would seem that a lot of thought needs to be given to proceeding to meniscal surgery.
Where Does Placebo Fit In?
With so much research being currently performed on neuroplasticity and the incredible power of the brain, the power of placebo just can’t be ignored. A placebo is an inert intervention: one that has no direct physiological explanation for working – like a salt pill, or sham surgery! Placebos typically have very few side effects (if any) when compared to prescription drugs, injections, or actual surgeries—and can at times work just as well.
Studies have shown that if you think you’re receiving a treatment, and you expect that treatment to work, it often does. In fact, the studies show around a third of people with placebo intervention will have resolution of symptoms. This was beautifully demonstrated in the Finnish study mentioned above—the sham knee surgery patients experienced the benefits in the same way as the real surgical patients did!. But how do placebos work? How can your brain produce healing just because you believe it should be happening?
Whilst the exact mechanisms of the placebo effect are not completely understood, it seems related to changes in your brain in response to different psychosocial stimuli. Not only can placeboeffects arise from a conscious belief in an intervention, but also from our subconscious associations between recovery and the experience of being treated—for example the simple physical experience of a treatment stimulates subconscious pathways that effect our recovery processes. This conditioned subconscious pathway means some body processes are controlled without us even being aware.
Exercise – Still The Best Intervention For Your Joints!
Exercise is the real medicine for pain in your joints. Exercise helps prevent and relieve joint pain through a number of mechanisms, including strengthening key stabilising muscles, improving flexibility and range of motion, flushing lubricating/synovial fluid through the joint, improving bone strength, and helping you keep your weight at optimal levels. The notion that exercise is detrimental to your joints is a serious misconception – there is no evidence to support this belief. It is simply a matter of finding the right exercises with the right technique, frequency and dosage!
So Where To From Here?
The Australian Orthopaedic Association (AOA) has a position statement on the use of arthroscopy in knee osteoarthritis, which is used to guide health professionals. While this clearly says this procedure has been shown to have no benefit for people with osteoarthritis, it does go on to list a series of things where it could be effective.
So whilst it’s becoming quite clear that a torn meniscus—at least, the wear-and-tear variety—is not going to be helped by a surgical trim, this does not necessarily mean that arthroscopic surgery has no role at all. Acute tears, loose bodies, and true physical locking of the knee may require an arthroscope in order for you to continue functioning. You just need to bear in mind that whilst removing the torn fragment may result in an immediate improvement in symptoms, you are losing some of that important shock absorbing cartilage that will almost inevitably result in some early arthritic development within your joint.
It also seems that the popularity of knee arthroscopes has resulted in many people taking this “quicker fix” rather than doing the things that they should be doing like managing their condition, whether that be losing weight, doing the right exercise,”
Remember that surgeries come with all sorts of risks, and there is no point in exposing yourself to these without some clear advantage, and strong evidence to support the benefit derived from the intervention.
References
Many references were used in the writing of this article, but the specific ones mentioned are listed below, with a few of the additional studies also listed at the end. We hope you enjoyed the article!
(1) http://www.nejm.org/doi/full/10.1056/NEJMoa013259
(2) http://www.nejm.org/doi/full/10.1056/NEJMoa1301408
(3) http://www.nejm.org/doi/full/10.1056/NEJMoa1305189?query=featured_home
(4) http://annals.org/article.aspx?articleid=2490532#.VsfPIxQm61Q.linkedin
http://articles.mercola.com/sites/articles/archive/2014/02/07/arthroscopic-knee-surgery.aspx
http://www.regenexx.com/should-i-have-meniscus-surgery/
http://www.abc.net.au/health/features/stories/2015/03/25/4203985.htm
https://stemcelldoc.wordpress.com/2008/09/24/meniscus-knee-surgery/